The walls of the upper floor of the abdominal cavity. Derivatives of the peritoneum in the upper floor of the abdominal cavity. The upper floor of the abdominal cavity. Clinical anatomy of the pancreas
The abdominal cavity is the part of the abdominal cavity covered by the parietal peritoneum. In men, it is closed, and in women it communicates with the uterine cavity through the openings of the fallopian tubes.
The visceral peritoneum covers the organs located in the abdominal cavity. Organs can be covered by the peritoneum on all sides (intraperitoneally), on three sides (mesoperitoneally) and extraperitoneally (on one side or lie extraperitoneally). The organs covered by the peritoneum intraperitoneally have significant mobility, which is increased by the mesentery or ligaments. The displacement of meso-peritoneal organs is insignificant (Fig. 123).
A feature of the peritoneum is that the mesothelium (the first layer of the peritoneum) forms a smooth surface that ensures the sliding of the organs during their peristalsis and changes in volume. In the peritoneal cavity, under normal conditions, there is a minimal amount of transparent serous fluid, which moisturizes the surface of the peritoneum and fills the gaps between organs and walls. The movements of organs in relation to each other and to the abdominal wall are made easily and without friction due to the fact that all contact surfaces are smooth and moist. Between the anterior wall of the abdomen and the internal organs there is a gasket-omentum. "
In the region of the diaphragm, the peritoneum becomes thinner at the site of the “suction hatches”. The lumen of the hatches changes during the respiratory movements of the diaphragm, which ensures their pumping action. "Suction hatches" are also present in the peritoneum of the rectovesical cavity in men and the recto-uterine cavity in women.
There are transuding, absorbing and indifferent to the abdominal fluid areas of the peritoneum. Transuding areas are the small intestine and broad ligaments of the uterus. The suction parts of the parietal peritoneum are the diaphragm and the iliac fossae.
The abdominal cavity of the mesentery of the transverse colon is divided into two floors: upper and lower, which communicate with each other in front through the preomental fissure and from the sides - through the right and left lateral canals. In addition, the peritoneal floor of the small pelvis is isolated
The upper floor of the abdominal cavity is located between the diaphragm and the mesentery of the transverse colon. It contains intraperitoneally covered stomach, spleen and mesoperitoneally - liver, gallbladder and upper part of duodenum. The pancreas belongs to the upper floor of the abdominal cavity, although it lies retroperitoneally, and part of the head is located below the root of the mesentery of the transverse colon. The listed organs, their ligaments and the mesentery of the transverse colon limit isolated spaces, cracks and bags in the upper floor of the abdominal cavity.
Top floor bags. The space between the diaphragm and the liver is divided by the falciform ligament into two sections: left and right.
The right liver bag, or bursa hepatica dextra, is the gap between the right lobe of the liver and the diaphragm. It is bounded above by the diaphragm, below by the right lobe of the liver, behind by the right part of the coronary ligament, and to the left by the falciform ligament of the liver. It distinguishes the right subdiaphragmatic space and subhepatic.
The right subphrenic space is located most deeply between the posterior surface of the right lobe of the liver, the diaphragm, and the coronary ligament. It is in the subdiaphragmatic space, as in the deepest place of the hepatic sac, that the fluid that has poured into the abdominal cavity can be retained. The subphrenic space in most cases directly passes into the right lateral canal of the lower floor of the abdominal cavity. Therefore, inflammatory exudate from the right iliac fossa can freely move towards the subphrenic space and lead to the formation of an encysted abscess, called a subphrenic abscess. It most often develops as a complication of perforated gastric and duodenal ulcers, destructive appendicitis, cholecystitis.
The subhepatic space is the lower section of the i fava of the hepatic sac and is located between the lower surface of the right lobe of the liver, the transverse colon and its mesentery, to the right of the gate of the liver and the hepatoduodenal ligament. In the subhepatic space, the anterior and posterior sections are distinguished. Almost the entire peritoneal surface of the gallbladder, the upper outer surface of the duodenum, faces the anterior part of this space. The posterior section, located at the posterior edge of the liver, is the least accessible part of the subhepatic space - a recess called the renal-hepatic pocket. Abscesses resulting from perforation of a duodenal ulcer or purulent cholecystitis are more often located in the anterior section, while the distribution of the periappendicular abscess occurs mainly in the posterior section of the subhepatic space.
The left subdiaphragmatic space consists of widely communicating bags: the left hepatic and pregastric.
The left hepatic bursa is a gap between the left lobe of the liver and the diaphragm, bounded on the right by the falciform ligament of the liver, behind the left part of the coronary ligament and the left triangular ligament of the liver. This bursa is much smaller in width and depth than the right hepatic bursa and is not usually identified as a distinct part of the subdiaphragmatic space.
The pregastric sac is bounded behind by the lesser omentum and stomach, the upper left lobe of the liver, the diaphragm, in front by the anterior abdominal wall, on the right by the falciform and round ligaments of the liver, on the left, the pregastric sac has no pronounced border. In the outer-posterior section of the left subdiaphragmatic space, the spleen is located with ligaments: gastrosplenic and diaphragmatic-splenic. () t of the left lateral canal, it is separated by the left phrenic-colic ligament. This ligament is often wide, it covers the lower pole of the spleen and is called the suspensory ligament of the spleen. Thus, the bed of the spleen is well demarcated from the left lateral canal, this is a blind pocket (saccus caecus lienalis). The left subdiaphragmatic space plays a much smaller role than the right one as a site of abscess formation. Purulent processes rarely developing in this space tend to spread between the left lobe of the liver and stomach down to the transverse colon or to the left to the blind sac of the spleen. Communication between the right hepatic and pregastric bags is carried out through a narrow gap between the liver and the pyloric part of the stomach, in front of the lesser omentum.
Stuffing bag (bursa omentalis) is a large closed slit-like space of the abdominal cavity, the most isolated and deep.
The anterior wall of the omental sac is formed by the lesser omentum, the posterior wall of the stomach, and the gastrocolic ligament (the initial part of the greater omentum). The lesser omentum is three ligaments that pass one into the other: hepatic-duodenal, hepatic-gastric and diaphragmatic-gastric. The lower wall of the omental sac is formed by the transverse colon and its mesentery. From above, the omental bag is bounded by the caudate lobe of the liver and the diaphragm, the posterior wall is formed by the parietal peritoneum, which covers the front of the pancreas, aorta, inferior vena cava, the upper pole of the left kidney with the adrenal gland, on the left it is limited by the spleen with the gastrosplenic ligament, and the right wall is not expressed.
In the omental bag, depressions or inversions are distinguished: the upper one is located behind the caudate lobe of the liver and reaches the diaphragm, the lower one is in the region of the mesentery of the transverse colon and the spleen.
Entry into the omental bag is possible only through the omental opening, bounded in front by the hepatoduodenal ligament, behind by the hepatorenal ligament, in the thickness of which lies the inferior vena cava, above by the caudate lobe of the liver, below by the renal-duodenal ligament.
The stuffing hole passes one or two fingers, but in case of adhesion formation it can be closed and then the stuffing bag is a completely isolated space. In the omental bag, the contents of the stomach can accumulate when the ulcer is perforated;
nigsya purulent processes as a result of inflammatory diseases of the pancreas.
There are three operational accesses to the stuffing bag for examination, revision of organs and operations on them (Fig. 124):
1. Through the gastrocolic ligament, which is most preferable, since it can be dissected widely. It is used to examine the posterior wall of the stomach and pancreas in case of inflammation and trauma.
2. Through the hole in the mesentery of the transverse colon in an avascular place, you can examine the cavity of the omental bag, apply a gastrointestinal anastomosis.
3. Access through the hepatogastric ligament is more convenient when the stomach is prolapsed. Used in operations on the celiac artery.
Channels and sinuses of the lower floor. The lower floor of the abdominal cavity occupies the space between the mesentery of the transverse colon and the small pelvis. The ascending and descending colons, the root of the mesentery of the small intestine divide the lower floor of the abdominal cavity into four sections: the right and left side canals and the right and left (mesenteric sinuses (Fig. 125).
The right lateral canal is located between the ascending colon and the right lateral wall of the abdomen. At the top, the canal passes into the subscapular space, at the bottom - into the right iliac fossa, and then into the small pelvis.
The left lateral canal is limited by the descending colon and the left lateral wall of the abdomen and passes into
left iliac region. The deepest in the horizontal position are the upper sections of the canals.
The right mesenteric sinus is limited to the right by the ascending colon, from above by the mesentery of the transverse colon, to the left and below by the mesentery of the small intestine. This sinus is largely delimited from other parts of the abdominal cavity. In the horizontal position, the upper right angle of the sinus is the deepest.
The left mesenteric sinus is larger than the right one. From above it is bounded by the mesentery of the transverse colon, on the left by the descending colon and the sigmoid mesentery, on the right by the mesentery of the small intestine. From below, the sinus is not limited and directly communicates with the pelvic cavity. In the horizontal position, the superior angle of the sinus is the deepest. Both mesenteric sinuses communicate with each other through a gap between the mesentery of the transverse colon and the initial part of the jejunum. Inflammatory exudate from the mesenteric sinuses may spread into the lateral channels of the abdominal cavity. The left mesenteric sinus is larger than the right one, and due to the absence of anatomical restrictions in its lower sections, suppurative processes that develop in the sinus tend to descend into the pelvic cavity much more often than from the right mesenteric sinus.
Along with the tendency for inflammatory exudates to spread through all the crevices of the abdominal cavity, there are anatomical prerequisites for the formation of encysted peritonitis both in the lateral canals and in the mesenteric sinuses, especially in the right one, as it is more closed. During operations on the abdominal organs, especially with peritonitis, it is important to divert the loops of the small intestine first to the left, then to the right and remove pus and blood from the mesenteric sinuses to prevent the formation of encysted abscesses.
Abdominal pockets. The peritoneum, passing from organ to organ, forms ligaments, next to which there are recesses, called pockets (recessus).
Recessus duodenojejunalis is formed at the junction of the duodenum into the jejunum, recessus iliocaecalis superior is formed at the confluence of the ileum into the caecum in the region of the upper iliac-caecal angle, recessus iliocaecalis inferior is formed in the region of the lower ileocecal angle, recessus retrocaecalis is located behind the caecum, recessus intersigmoideus - a funnel-shaped depression between the mesentery of the sigmoid colon and the parietal peritoneum, its beginning faces the left lateral canal.
Peritoneal pockets can become the site of internal hernia formation. Peritoneal pockets with internal hernias can reach very large sizes. Internal hernias can become strangulated and cause intestinal obstruction.
Topographic anatomy of the stomach. The stomach is the main organ of the digestive system and is a mystical sac-like extension of the digestive tract located between the esophagus and the duodenum.
Holotopia. The stomach is projected onto the anterior abdominal wall in the left hypochondrium and its own epigastric region.
Departments. The inlet of the stomach is called cardiac, and the outlet is called pyloric. The perpendicular, descending from the esophagus to the greater curvature, divides the stomach into a cardial section, consisting of the fundus and body, and a pyloric section, consisting of the vestibule and pyloric canal. In the stomach, there is a greater and lesser curvature, anterior and posterior surfaces.
Syntopy. The concept of "syntopic fields of the stomach" is distinguished. These are the places where the stomach comes into contact with neighboring organs. Syntopic fields of the stomach must be taken into account in case of combined wounds, penetration of ulcers and germination of stomach tumors. Three syntopic fields are distinguished on the anterior wall of the stomach: hepatic, diaphragmatic and free, which is in contact with the anterior wall of the abdomen. This field is also called the gastric triangle. This site is commonly used for gastrotomies and gastrostomies. The size of the gastric triangle depends on the filling of the stomach. Five syntopic fields are distinguished on the posterior wall of the stomach: splenic, renal, adrenal, pancreatic, and gastrointestinal.
Position. In the abdominal cavity, the stomach occupies a central position in the upper floor. Most of the stomach is located in the left subphrenic space, limiting the pancreatic sac in the back and the omental sac in front. The position of the stomach corresponds to the degree of inclination of the longitudinal axis of the stomach. Shevkunenko, in accordance with the location of the axis of the stomach, identified three types of positions: vertical (hook shape), horizontal (horn shape), oblique. It is believed that the position of the stomach is directly dependent on the type of physique.
relation to the peritoneum. The stomach occupies an intraperitoneal position. In places of transition of the sheets of the peritoneum on the lesser and greater curvature, ligaments of the stomach are formed. Ligaments of the stomach are divided into superficial and deep. Surface bonds:
1) gastrocolic (part of the greater omentum);
2) gastro-splenic, short gastric vessels pass through it, splenic vessels are located behind the ligament;
3) gastro-diaphragmatic;
4) diaphragmatic-esophageal, in it passes the esophageal branch from the left gastric artery;
5) hepatogastric, in it along the lesser curvature is the left gastric artery and vein;
6) hepato-pyloric - continuation of the hepatic / laryngeal ligament. It has the form of a narrow strip stretched between the gates of the liver and the pylorus, is an intermediate part between the hepatic-gastric and hepato-duodenal in dogs and serves as the right border when dissecting the ligaments of the stomach.
Deep Ligaments:
1) gastro-pancreas (during the transition of the peritoneum from the upper-I icro edge of the pancreas to the posterior surface of the stomach);
2) with pyloric-pancreas (between the pyloric otic um of the stomach and the right side of the body of the pancreas);
3) lateral diaphragmatic-piciform.
Blood supply of the stomach. The stomach is surrounded by a ring
wide anastomosing vessels giving off intramural branches and forming a dense network in the submucosa (Fig. 126). The source of blood supply is the celiac trunk, from which the left gastric artery departs, which goes directly to the lesser curvature of the stomach. The right gastric artery departs from the common hepatic artery, which anastomoses with the left on the lesser curvature of the stomach, forming an arterial arc of the lesser curvature. The left and right gastroepiploic arteries form an arc of greater curvature, and there are also short gastric arteries.
Innervation of the stomach. The stomach has a complex nervous apparatus. The main sources of innervation are the vagus nerves, the celiac plexus and its derivatives: gastric, hepatic, splenic, superior mesenteric plexus. The vagus nerves, branching on the esophagus, form the esophageal plexus, I de branches of both nerves are mixed and repeatedly connected. Passing from the esophagus to the stomach, the branches of the esophageal plexus are concentrated into several trunks: the left one passes to the anterior surface of the stomach, and the right one to the posterior surface of the stomach, giving branches to the liver, solar plexus, kidney and other organs. A long branch of Latarjet departs from the left vagus nerve to the pyloric section of the stomach. vagus nerves are a complex conduction system that connects nerve fibers of various functional purposes to the stomach and other organs. Between the left and right nerves there are a large number of connections in the chest and abdominal cavities, here there is an exchange of fibers. Therefore, it is impossible to talk about the exclusive innervation of the anterior wall of the stomach by the left vagus nerve, and the posterior wall by the right one. The right vagus nerve goes more often in the form of a single trunk, and the left one forms from one to four branches, more often there are two.
Lymph nodes of the stomach. Regional lymph nodes of the stomach are located along the lesser and greater curvature, as well as along the left gastric, common hepatic, splenic and celiac arteries. According to A. V. Melnikov (1960), lymph outflow from the stomach occurs through four main collectors (pools), each of which includes 4 stages.
Collector I of the lymphatic outflow collects lymph from the pyloric-angral part of the stomach, adjacent to the greater curvature. The first stage is the lymph nodes located in the thickness of the gastrocolic ligament along the greater curvature, near the pylorus, the second stage is the lymph nodes along the edge of the pancreatic head under and behind the pylorus, the third stage is the lymph nodes located in the thickness of the mesentery of the small intestine , and the fourth - retroperitoneal para-aortic lymph nodes.
In the 7/ collector of the lymphatic outflow, lymph flows from the part of the pyloric-antral section adjacent to the lesser curvature, and partly from the body of the stomach. The first stage is the retropyloric lymph nodes, the second is the lymph nodes in the lesser omentum in the dietary part of the lesser curvature, in the region of the pylorus and duodenum, immediately behind the pylorus, the third stage is the lymph nodes located in the thickness of the hepatic o-gastric ligament. The fourth stage A. V. Melnikov considered the lymph nodes in the gates of the liver.
Collector III collects lymph from the body of the stomach and lesser curvature, adjacent sections of the anterior and posterior walls, paintings, the medial part of the fornix and the abdominal esophagus. The first stage is the lymph nodes located in the form of a chain along the lesser curvature in the fiber of the lesser omentum. The upper nodes of this chain are called paracardial; in cancer of the cardia, they are affected by metastases in the first place. Lymph nodes along the left gastric vessels, in the thickness of the gastro-pancreatic ligament, are the second stage. I third stage - lymph nodes along the upper edge of the pancreas and in the region of its tail. The fourth stage is the lymph nodes in the paraesophageal tissue above and below the diaphragm.
In the IV collector, lymph flows from the vertical part of the greater curvature of the stomach, the adjacent anterior and posterior walls, and a significant part of the fornix of the stomach. Lymph nodes located in the upper left gastrocolic ligament are the first stage. The second stage is the lymph nodes along the short arteries of the stomach, the third stage is the lymph nodes in the hilum of the spleen. A. V. Melnikov considered the defeat of the spleen to be the fourth stage.
Knowledge of the anatomy of the regional lymph nodes of all collectors is extremely important for the correct operation of the stomach in compliance with oncological principles.
Topographic anatomy of the duodenum. The duodenum (duodenum) is the initial section of the small intestine. In front, it is covered by the right lobe of the liver and the mesentery of the transverse colon, it itself covers the head of the pancreas, so the duodenum lies deep and does not directly adjoin the anterior abdominal wall anywhere. The duodenum is divided into four parts. It consists of upper horizontal, descending, lower horizontal and ascending parts. Knowing the syntopy of the duodenum helps to explain the direction of penetration of the ulcer, the germination of the tumor and the spread of phlegmon during retroperitoneal rupture of the organ.
The upper part of the duodenum, 4-5 cm long, is located between the pylorus and the upper flexure of the duodenum and goes to the right and back along the right surface of the spine, passing into the descending part. This is the most mobile section of the intestine, covered on all sides by the peritoneum. All other sections of the intestine are covered with peritoneum only in front. In the initial section of the duodenum, an extension is determined, which is called the duodenal bulb. The upper part of the duodenum from above; in contact with the square lobe of the liver, in front - with the gallbladder, behind - with the portal vein, gastroduodenal artery, common bile duct. From below and from the inside, the head of the pancreas is adjacent to the intestine.
The descending part of the duodenum, 10-2 cm long, is located between the flexura duodeni superior and flexura duodeni inferior. This part of the duodenum is inactive and is covered by the peritoneum only in front. The descending part of the duodenum in front borders on the right lobe of the liver, the mesentery of the transverse colon, behind - on the gate of the right kidney, renal pedicle, inferior vena cava. Outside, the ascending part and the hepatic flexure of the colon are adjacent, from the inside, the head of the pancreas. The common bile duct and the pancreatic duct open into the descending part of the duodenum. They perforate the postero-meshal wall of the descending part of the duodenum in its middle section and open on the major (vater) papilla of the duodenum. Above it, there may be a non-permanent small duodenal papilla, on which the accessory pancreatic duct opens.
From the lower bend of the duodenum begins - 1 "and its horizontal part 2 to 6 cm long, covered in front by the peritoneum. The horizontal (lower) part lies at the level of the III and IV lumbar vertebrae, below the mesentery of the transverse colon, partly behind the root of the mesentery of the small intestine The first oriental part of the duodenum passes into the ascending part, 6-10 cm long. in front - the transverse colon, loops of the racent intestines, the root of the mesentery of the small intestines and superior mesenteric vessels.Behind - the right psoas muscle, inferior vena cava, aorta, left renal vein.
Tie the duodenum. The hepatoduodenal ligament is located between the hilum of the liver and the initial Hi (fracture of the upper part of the duodenum. It fixes the I initial section of the intestine and limits the omental opening< переди. В связке располагаются: общий желчный проток справа, | обственная печеночная артерия слева, а между ними и сзади - поротная вена. Двенадцатиперстно-почечная связка в виде склад- Mi брюшины натянута между наружным краем нисходящей части шенадцатиперстной кишки и правой почкой, где она переходит в париетальную брюшину, расположенную кпереди от почки. Она 01 раничивает сальниковое отверстие снизу. Большую роль в фик- i.iiшп двенадцатиперстно-тощекишечного изгиба играет связка I рейтца (lig. duodenojejunalis).
In the upper part of the duodenum is covered with peritoneum from ■ h ex sides. The descending and horizontal parts are located retroperitoneally, the ascending part occupies an intraperitoneal position.
The blood supply of the duodenum (see Fig. 126) I a "streaks from the system of the celiac trunk and the superior mesenteric irgern. The upper and lower pancreatic-duodenal arteries have anterior and posterior branches. As a result of anastomosis, anterior and posterior arterial arches are formed between them, which go between the concave semicircle of the duodenum and the head of the pancreas, which makes it impossible to separate them during surgery and forces them to be removed as a single block - pancreatoduodenal resection, performed, for example, in cancer of the Vater nipple or tumor of the pancreatic head.
Large glands of the digestive tract
Topographic anatomy of the liver. The liver is one of the large glands in the digestive tract. The liver is distinguished by four morphofunctional features: 1) is the largest organ; 2) has three circulatory systems: arterial, venous and portal; 3) all substances that enter the gastrointestinal tract pass through it; 4) serves as a huge blood depot; 5) participates in all types of metabolism, synthesizes albumins, globulins, factors of the blood coagulation system, plays an important role in carbohydrate and fat metabolism and detoxification of the body, plays an important role in lymph production and lymph circulation.
Gayutopia. The liver of an adult is located in the right hypochondrium, the epigastric region proper, and partially in the left hypochondrium. The projection of the liver on the anterior abdominal wall looks like a triangle and can be built on three points: the upper point is on the right at the level of the 5th costal cartilage along the midclavicular line, the lower point is the 10th intercostal space along the midaxillary line, on the left - at the level of 6- th costal cartilage along the parasternal line. The lower border of the liver coincides with the costal arch. Behind the liver is projected onto the chest wall, to the right of the 10-11th thoracic vertebrae.
The position of the liver. The liver in relation to the frontal plane can be located: 1) in the dorsopetal position, the diaphragmatic surface of the liver is thrown back and its front edge can be located above the costal arch; 2) in the ventropetal position, the diaphragmatic surface faces forward, and the visceral surface faces backwards. In the ventropetal position, surgical access to the lower surface of the liver is difficult, and in the dorsopetal position, to the upper one.
The liver can occupy a right-sided position, then its right lobe is highly developed, and the size of the left lobe is reduced. () the organ occupies an almost vertical position, sometimes located only in the right half of the abdominal cavity. The left-sided position of the liver is characterized by the location of the organ in the horizontal plane and with a well-developed left lobe, which in some cases can go beyond the spleen.
Syntopy of the liver. The diaphragmatic surface of the right juli of the liver borders on the pleural cavity, the left lobe - on the pericardium, from which it is separated by the diaphragm. The visceral surface of the liver comes into contact with various organs, from which depressions form on the surface of the liver. The left lobe of the liver borders the lower end of the esophagus and the stomach. The pyloric part of the stomach is adjacent to the square lobe. The right lobe of the liver in the region of the neck of the gallbladder adjoins the upper horizontal part of the duodenum. 11 to the right is in contact with the transverse colon and the hepatic curvature of the colon. Posterior to this impression, the surface of the right lobe of the liver borders the right kidney and adrenal gland. Syntopy of the liver must be taken into account when assessing possible options for combined injuries of the abdominal and thoracic cavities.
The gate of the liver is an anatomical formation, which is made up of the transverse and left longitudinal grooves of the visceral surface of the liver. Here, vessels and nerves enter the liver and bile ducts and lymphatic vessels exit. In the gates of the liver, the vessels and ducts are accessible for surgical treatment, since they are located superficially, outside the parenchyma of the organ. Of practical importance is the shape of the gate: open, closed and intermediate. With an open form of the gate of the liver, the transverse sulcus communicates with the left sagittal and accessory sulci, thereby creating favorable conditions for access to the lobar and segmental ducts. With a closed form of the gate of the liver, there is no communication with the left sagittal sulcus, there are no additional grooves, the size of the gate is reduced, therefore, it is impossible to isolate segmental vessels and ducts in the gate of the liver without dissecting its perenchyma.
The gates of the liver can be located in the middle between the edges of the liver or shifted to its posterior or anterior edge. In the case of posterior displacement of the gate, more difficult conditions are created for prompt access to the vessels and ducts of the portal system during liver resections and operations on the biliary tract.
The relation to the peritoneum is mesoperitoneal, that is, the liver is covered with peritoneum on three sides. The posterior surface of the liver is not covered by the peritoneum, it is called the extraperitoneal field of the liver or pars m.ida.
The ligamentous apparatus of the liver is usually divided into true ligaments and peritoneal ligaments. True ligaments: 1) coronary, firmly fixing the posterior surface of the liver to the diaphragm, turning into triangular ligaments at the edges; 2) sickle-shaped, located in the sagittal plane at the border of the right and left lobes and turning into a steep ligament, which goes to the navel and contains a partially obliterated umbilical vein. From the visceral surface of the liver, the peritoneal ligaments are sent down to the organs: hepatogastric and hepatoduodenal. The hepatoduodenal ligament (ligament of life) is considered the most important, since the common bile duct (on the right), the common hepatic artery (on the left) and the portal vein pass through it, lies between them and posteriorly. Clamping of the hepatoduodenal ligament with fingers or a special instrument is used to temporarily stop bleeding from the liver.
Fixing apparatus of the liver. The liver is kept in the correct anatomical position: 1) extraperitoneal field (part of the posterior surface of the liver, not covered by the peritoneum); 2) the inferior vena cava, lying on the posterior surface of the liver and receiving the hepatic veins. Above the liver, the vein is fixed in the opening of the diaphragm, below it is firmly connected with the spine; 3) intra-abdominal pressure, muscle tone of the anterior abdominal wall and suction action of the diaphragm; 4) ligaments of the liver.
Blood supply to the liver. Two vessels bring blood to the liver: the hepatic artery and the portal vein, respectively 25 and 75%. The arterial supply of the liver comes from the common hepatic artery, which, after departing from it by the gastroduodenal artery, is called the proper hepatic artery and is divided into the right and left hepatic arteries.
Portal vein, v. porta, is formed behind the head of the pancreas. This is the first section of the vein, which is called the pars pancreatica. The second section of the portal vein is located behind the upper horizontal part of the duodenum and winds pars retroduodenalis. The third section of the vein is located in the head of the hepatoduodenal ligament above the upper horizontal part of the duodenum and is called pars supraduodenaiis. The portal vein collects blood from unpaired organs of the abdominal cavity: intestines, spleen, stomach, and is formed from three large trunks: the splenic vein, superior mesenteric and inferior mesenteric veins.
At the hilum of the liver, the hepatic artery, portal vein, and bile duct form the portal triad, Glisson's triad.
Liver jen, vv. hepatic i, are collected from the central lobular veins and, ultimately, form three large trunks, the right, left and middle hepatic veins, which emerge from the liver tissue on the posterior surface at the upper edge (caval portal of the liver) and flow into the inferior vena cava vein at the level of its transition through the diaphragm.
The structure of the liver, segmental division. The division of the liver into right, left, caudate and square lobes, accepted in classical anatomy, is unacceptable for surgery, since the outer boundaries of the lobes do not correspond to the internal architectonics of the vascular and biliary systems. The modern division of the liver into segments is based on the principle of coincidence of the course of the first-order branches of the three liver systems: portal, arterial and bile, as well as the location of the main venous trunks of the liver. The portal vein, hepatic artery, and bile ducts are called the portal system (portal triad, Glisson triad). The course of all elements of the portal system inside the liver is relatively the same. The hepatic veins are called the caval system. The course of the vessels and bile ducts of the portal system of the liver does not coincide with the direction of the vessels of the caval system. Therefore, division of the liver according to the portal sign is now more common. The division of the liver along the portal system is of greater importance for the surgeon, since it is with the isolation and ligation of the vascular-secretory elements in the gates of the liver that the resection of this organ begins. However, when performing a resection based on liver division along the portal system, it is necessary to take into account the course of the hepatic veins (caval system) so as not to disturb the venous outflow. In clinical practice, the scheme of segmental division of the liver according to Quino, 1957 (Fig. 127) has become widespread. According to this scheme, the liver is divided into two lobes, five sectors and eight segments. The segments are arranged in radii around the gate. Lobe, sector and segment is called a section of the liver, which has separate blood supply, bile outflow, innervation and lymph circulation. The lobes, sectors and segments of the liver are separated from each other by four main gaps.
 |
Abdomen ( cavitas abdominis) - a space bounded at the top by the diaphragm, at the bottom - by the cavity of the small pelvis, behind - by the lumbar spine with the square muscles of the lower back adjacent to it, the iliopsoas muscles, in front and from the sides - by the abdominal muscles.
In the abdominal cavity are the digestive organs (stomach, small and large intestines, liver, pancreas), spleen, kidneys, adrenal glands and ureters, blood vessels and nerves.
The inner surface of the abdominal cavity is lined internally by the abdominal fascia ( fascia endoabdominalis), medially from which the peritoneum is located.
Scheme of the relationship of organs to the peritoneum (cross section)
Peritoneum ( peritoneum) - a serous membrane lining the walls of the abdominal cavity (parietal sheet of the peritoneum) and internal organs (visceral sheet of the peritoneum). Between the visceral and parietal layers of the peritoneum is the peritoneal cavity ( cavitas peritonei). The peritoneum secretes a serous fluid, which moisturizes it and ensures the free sliding of the organs covered with the peritoneum:
1- peritoneum parietale- parietal peritoneum - covers the walls of the abdominal cavity;
2 - peritoneum viscerale- visceral peritoneum, which differently covers the organ;
3 - mesoperitoneal position. The organ is covered by the peritoneum on three sides (eg, ascending and descending colon, liver);
4 - extraperitoneal position. The organ is covered by the peritoneum on one side (for example, the pancreas and part of the duodenum) or not covered at all (for example, the kidney), which is called the retroperitoneal position;
5 - intraperitoneal position. The organ is covered with peritoneum on all sides (for example, the stomach, the mesenteric part of the small intestine);
6 - mesenterium- mesentery of the small intestine;
7 -cavitas peritonei- peritoneal cavity.
Scheme of the course of the peritoneum on the sagittal section (in men)

The peritoneum, passing from the walls of the abdominal cavity to the organs and when moving from organ to organ, forms ligaments, which are a duplicate of the peritoneum (two sheets):
1 -lig. coronarium hepatis- the coronary ligament of the liver, which is formed during the transition of the peritoneum from the diaphragm to the liver;
2 - hepar- liver - mesoperitoneally covered with peritoneum. The peritoneum passes from the visceral surface of the liver to the duodenum ( lig. hepatoduodenale) and lesser curvature of the stomach ( lig. hepatogastricum);
3 - lig. hepatogastricum- hepatogastric ligament, which, together with lig. hepatoduodenale forms a small omentum ( omentum minus). Behind the lesser omentum and stomach is the stuffing bag;
4 - bursa omentalis - stuffing bag - limited: above - by the caudate lobe of the liver, below - by the posterior plate of the greater omentum or, taken as a whole, by the mesentery of the transverse colon, in front - by the stomach and lesser omentum, behind - by the parietal peritoneum and the organs that it covers ( v. cava inferior, aorta, corpus pancreatis);
5-gaster- stomach - covered with peritoneum intraperitoneally. At the point of transition lig. hepatoduodenale on the stomach between the two layers of the peritoneum and the lesser curvature of the stomach there is an area not covered by the peritoneum, or a bare spot;
6- pars nuda (curvatura ventriculi minor) - a bare place (small curvature of the stomach);
7- pars nude (curvatura ventriculi major) - a bare place (greater curvature of the stomach). Along the greater curvature of the stomach, two sheets of peritoneum are connected and descend down in front of the transverse colon and loops of the small intestine (the anterior plate of the greater omentum). Then these two sheets of peritoneum are tucked backwards and rise up (the posterior plate of the greater omentum). Thus, a large omentum is formed from the four sheets of the peritoneum.
8 - omentum majus- big omentum. The posterior plate of the greater omentum (two posterior layers of the peritoneum) goes to the posterior abdominal wall and splits. One sheet passes to the back wall of the peritoneal cavity, the other - to the transverse colon, connecting with another sheet of the peritoneum - the mesentery of the transverse colon is formed, which, thus, will consist of four sheets of peritoneum;
9- mesocolon transversum- mesentery of the transverse colon;
10 - colon transverse- transverse colon - covered by the peritoneum intraperitoneally. The lower sheet of the mesentery of the transverse colon passes to the posterior wall of the peritoneal cavity. The pancreas and most of the duodenum are located retroperitoneally (extraperitoneally);
11 - pancreas- pancreas;
12 - duodenum- duodenum - parietal peritoneum, covering the front side of the duodenum; passes to the small intestine. Its two leaves form the mesentery of the small intestine;
13 - mesenterium- mesentery of the small intestine;
14 - jejunum- jejunum - located in relation to the peritoneum intraperitoneally; has one bare spot ( pars nude) in the area of attachment of the mesentery;
15 - rectum- rectum;
16 - vesica urinaria- urinary bladder;
17- spatium retroperitoneale- retroperitoneal space - filled with fatty tissue. It contains the kidneys and ureters;
18 - excavatio rectovesicale- rectovesical deepening;
19 - os pubis- pubic bone.
TOPOGRAPHICAL ANATOMY OF THE UPPER ABDOMINAL CAVITY
The abdominal cavity is a space lined from the inside by intra-abdominal fascia.
Borders: above - the diaphragm, below - the boundary line, in front - the anterolateral wall, behind - the posterior wall of the abdomen.
Departments:
abdominal (peritoneal) cavity - a space limited by the parietal sheet of the peritoneum;
retroperitoneal space - the space located between the parietal peritoneum and the intra-abdominal fascia, which lines the back wall of the abdomen from the inside.
Peritoneum
The peritoneum is a serous membrane that lines the walls of the abdomen from the inside and covers most of its organs. Departments:
parietal(parietal) peritoneum– lines the walls belly.
Visceral peritoneum– covers the organs of the abdominal cavity.
Options for covering organs with peritoneum:
intraperitoneal - from all sides; mesoperitoneal - on three sides (one side is not
covered); extraperitoneal - on the one hand.
Properties of the peritoneum : humidity, smoothness, shine, elasticity, bactericidal, adhesiveness.
Functions of the peritoneum : fixing, protective, excretory, absorbing, receptor, conductive, depositing (blood).
Course of the peritoneum
From the anterior abdominal wall, the peritoneum passes to the lower concave surface of the diaphragm, then to the upper surface.
the surface of the liver and forms two ligaments: one in the sagittal plane - sickle-shaped, the second in the frontal plane - the coronary ligament of the liver. From the upper surface of the liver, the peritoneum passes to its lower surface and, approaching the gates of the liver, meets with a leaf of the peritoneum, which goes to the liver from the posterior abdominal wall. Both sheets go to the lesser curvature of the stomach and the upper part of the duodenum, forming a lesser omentum. Covering the stomach from all sides, the leaves of the peritoneum descend from its large curvature and, turning, return and approach in front of the transverse colon to the body of the pancreas, forming a greater omentum. In the region of the body of the pancreas, one sheet of current rises up, forming the posterior wall of the abdominal cavity. The second sheet goes to the transverse colon, covers it from all sides, returns back, forming the mesentery of the intestine. Then the sheet goes down, covers the small intestine from all sides, forms its mesentery and the mesentery of the sigmoid colon and descends into the pelvic cavity.
Floors of the abdomen
The peritoneal cavity of the transverse colon and its mesentery is divided into two floors:
Top floor– located above the transverse colon intestines and its mesentery. Contents: liver, spleen, stomach, partially duodenum; right and left hepatic, subhepatic, pregastric and omental bursae.
lower floor– located below the transverse colon intestines and its mesentery. Contents: loops of the jejunum and sub-ileum; caecum and appendix;
colon; lateral canals and mesenteric sinuses. The root of the mesentery of the transverse colon goes from right to left from the right kidney, slightly below its middle, towards the middle of the left. On its way, it crosses: the middle of the descending part of the duodenum; the head of the pancreas
noah gland and goes along the upper edge of the body of the gland.
Bags of the upper floor of the abdominal cavity
Right liver bag located between the diaphragm and the right lobe of the liver and is limited behind the right coronary
a ligament of the liver, on the left - a falciform ligament, and on the right and below it opens into the subhepatic sac and the right lateral canal.
Left hepatic sac lies between the diaphragm and the left lobes of the liver and is bounded behind the left coronary ligament of the liver, on the right - by the falciform ligament, on the left - by the left triangular ligament of the liver, and in front it communicates with the pancreatic sac.
Pregastric bag located between the stomach and the left lobe of the liver and is bounded in front by the lower surface of the left lobe of the liver, behind - by the lesser omentum and the anterior wall of the stomach, from above - by the gates of the liver and communicates with the subhepatic sac and the lower floor of the abdominal cavity through the preomental fissure.
Subhepatic bag limited in front and above by the lower surface of the right lobe of the liver, below - by the transverse colon and its mesentery, on the left - by the gates of the liver and on the right opens into the right lateral canal.
Stuffing bag forms a closed pocket behind stomach and consists of vestibule and gastro-pancreatic sac.
The vestibule of the omental bag bounded at the top of the tail
that lobe of the liver, in front - a small omentum, from below - the duodenum, behind - the parietal part of the peritoneum lying on the aorta and the inferior vena cava.
Stuffing hole limited in front by the hepatoduodenal ligament, in which the hepatic artery, common bile duct and portal vein are laid, from below - by the duodenal-renal ligament, from behind - by the hepato-renal ligament, from above - by the caudate lobe of the liver.
Gastrointestinal- pancreatic sac limited front to rear
the surface of the lesser omentum, the posterior surface of the stomach and the posterior surface of the gastrocolic ligament, behind - the parietal peritoneum lining the pancreas, aorta and inferior vena cava, above - the caudate lobe of the liver, below - the mesentery of the transverse colon, on the left - the stomach -dochno-splenic and renal-splenic ligaments.
Topographic anatomy of the stomach Holotopia: left hypochondrium, actually epigastric ob-
Skeletotopia:
cardiac opening - to the left of Th XI (behind the cartilage of the VII rib);
bottom - Th X (V rib along the left midclavicular line); gatekeeper - L1 (VIII right rib in the midline).
syntopia: above - the diaphragm and the left lobe of the liver, behind
on the left - the pancreas, left kidney, adrenal gland and spleen, in front - the abdominal wall, below - the transverse colon and its mesentery.
Ligaments of the stomach:
Hepatic- gastric ligament– between the gates of the liver and lesser curvature of the stomach; contains the left and right gastric arteries, veins, branches of the vagus trunks, lymphatic vessels and nodes.
diaphragmatic- esophageal ligament– between the diaphragm
esophagus and cardial part of the stomach; contains a branch of the left gastric artery.
Gastrointestinal- diaphragmatic ligament formed as a result the transition of the parietal peritoneum from the diaphragm to the anterior wall of the fundus and partially to the cardial part of the stomach.
Gastrointestinal- splenic ligament– between the spleen and greater curvature of the stomach; contains short arteries and veins of the stomach.
Gastrointestinal- colonic ligament– between the greater curvature stomach and transverse colon; contains the right and left gastroepiploic arteries.
Gastrointestinal- pancreatic ligament formed during the transition
de peritoneum from the upper edge of the pancreas to the back wall of the body, cardia and fundus of the stomach; contains the left gastric artery.
Blood supply to the stomach provided by the celiac trunk system.
Left gastric artery is divided into ascending esophageal and descending branches, which, passing along the lesser curvature of the stomach from left to right, give off the anterior and posterior branches.
Right gastric artery starts from own hepatic artery. As part of the hepatoduodenal ligament, the artery reaches the pyloric
of the stomach and between the leaves of the lesser omentum along the lesser curvature goes to the left towards the left gastric artery, forming an arterial arc of the lesser curvature of the stomach.
Left gastrointestinal- omental artery is a branch splenic artery and is located between the sheets of the gastro-splenic and gastrocolic ligaments along the greater curvature of the stomach.
Right gastrointestinal- omental artery starts from gastroduodenal artery and goes from right to left along the greater curvature of the stomach towards the left gastroepiploic artery, forming a second arterial arch along the greater curvature of the stomach.
short gastric arteries in quantity 2-7 branches depart from the splenic artery and, passing in the gastrosplenic ligament, reach the bottom along the greater curvature
The veins of the stomach accompany the arteries of the same name and flow into the portal vein or into one of its roots.
Lymph drainage
The efferent lymphatic vessels of the stomach flow into the lymph nodes of the first order, located in the lesser omentum, located along the greater curvature, at the gates of the spleen, along the tail and body of the pancreas, into the subpyloric and superior mesenteric lymph nodes. The efferent vessels from all the listed first-order lymph nodes are sent to the second-order lymph nodes, which are located near the celiac trunk. From them, the lymph flows into the lumbar lymph nodes.
Innervation of the stomach provided by the sympathetic and parasympathetic parts of the autonomic nervous system. The main sympathetic nerve fibers are sent to the stomach from the celiac plexus, enter and spread in the organ along the extra- and intraorganic vessels. Parasympathetic nerve fibers enter the stomach from the right and left vagus nerves, which form the anterior and posterior vagus trunks below the diaphragm.
Topographic anatomy of the duodenum Holotopia: in the epigastric and umbilical regions.
The duodenum is divided into four sections: superior, descending, horizontal, and ascending.
Top part ( bulb ) duodenum located between the pylorus and the superior flexure of the duodenum.
Relation to the peritoneum: covered intraperitoneally in the initial, mesoperitoneally in the middle parts.
Skeletotopia– L1.
syntopia: above the gallbladder from below the head of the pancreas, in front of the antrum of the stomach.
Descending part duodenum forms more or less pronounced bend to the right and goes from the upper to the lower bends. The common bile duct and the pancreatic duct on the major duodenal papilla open into this part. A little above it, there may be a non-permanent small duodenal papilla, on which an additional pancreatic duct opens.
Relation to the peritoneum:
Skeletotopia– L1-L3.
syntopia: on the left is the head of the pancreas, behind and on the right, the right kidney, right renal vein, inferior vena cava and ureter, in front of the mesentery of the transverse colon and loops of the small intestine.
horizontal part duodenum goes from the lower bend to the intersection with the superior mesenteric vessels.
Relation to the peritoneum: located retroperitoneally.
Skeletotopia– L3.
syntopia: from above the head of the pancreas, behind inferior vena cava and abdominal aorta, in front and below the loop of the small intestine.
ascending part of the duodenum goes from the intersection with the superior mesenteric vessels to the left and up to the duodeno-jejunal flexure and is fixed by the suspensory ligament of the duodenum.
Relation to the peritoneum: located mesoperitoneally.
Skeletotopia– L3-L2.
syntopia: from above the lower surface of the body of the pancreas, behind the inferior vena cava and abdominal aorta, in front and below the loop of the small intestine.
Ligaments of the duodenum
Hepatic- duodenal ligament– between the gates liver and the initial section of the duodenum and contains its own hepatic artery, located in the ligament on the left, the common bile duct, located on the right, and between them and behind - the portal vein.
duodenal- renal ligament in the form of a fold
the tires are stretched between the outer edge of the descending part of the intestine and the right kidney.
Blood supply to the duodenum provide
is derived from the system of the celiac trunk and the superior mesenteric artery.
Posterior and anterior superior pancreas- twelve-
duodenal arteries depart from the gastroduodenal arteries.
rear and anterior inferior pancreas-
duodenal arteries arise from the superior mesenteric arteries, go towards the top two and connect with them.
The veins of the duodenum repeat the course of the arteries of the same name and divert blood into the portal vein system.
Lymph drainage
The efferent lymphatic vessels empty into the lymph nodes of the first order, which are the upper and lower pancreaticoduodenal nodes.
innervation The duodenum is carried out from the celiac, superior mesenteric, hepatic and pancreatic nerve plexuses, as well as branches of both vagus nerves.
Intestinal suture
Intestinal suture is a collective concept that combines all types of sutures that are applied to hollow organs (esophagus, stomach, small and large intestines).
Primary requirements, presented to the intestinal suture:
tightness– is achieved by contact of the serous membranes of the stitched surfaces.
Hemostatic– is achieved by capturing the submucosal base of the hollow organ into the suture (the suture should provide hemostasis, but without significant disruption of the blood supply to the organ wall along the suture line).
adaptability– the seam must be carried out taking into account sheath structure of the walls of the digestive tract for optimal comparison with each other of the same name shells of the intestinal tube.
Strength– is achieved by capturing the submucosal layer in the seam, where a large number of elastic fibers are located.
Asepsis(purity, uninfected) - this requirement is met if the mucosa of the organ is not captured in the suture (the use of “clean” single-row sutures or the immersion of through (infected) sutures with a “clean” serous-muscular suture).
In the wall of the hollow organs of the abdominal cavity, four main layers are distinguished: the mucous membrane; submucosal layer; muscle layer; serous layer.
The serous membrane has pronounced plastic properties (the surfaces of the serous membrane brought into contact with the help of sutures after 12-14 hours are firmly glued together, and after 24-48 hours the connected surfaces of the serous layer are firmly fused with each other). Thus, suturing, bringing together the serous membrane, ensures the tightness of the intestinal suture. The frequency of such seams should be at least 4 stitches per 1 cm of the length of the stitched area. The muscular coat gives elasticity to the suture line and therefore its capture is an indispensable attribute of almost any type of intestinal suture. The submucosal layer provides the mechanical strength of the intestinal suture, as well as good vascularization of the suture zone. Therefore, the connection of the edges of the intestine is always produced with the capture of the submucosa. The mucous membrane does not have mechanical strength. The connection of the edges of the mucous membrane provides a good adaptation of the edges of the wound and protects the suture line from the penetration of infection from the lumen of the organ.
Classification of intestinal sutures
Depending on the application method
manual;
mechanical– superimposed by special devices;
combined.
Depending on whether , which layers of the wall are captured - in a seam
gray- serous; serous- muscular;
slimy- submucosal; seriously- muscular- submucosal;
serous- muscular- submucosally- mucous(through).
Through seams are infected ("dirty").
Sutures that do not pass through the mucous membrane are called non-infected (“clean”).
Depending on the row of intestinal sutures
single row seams(Bira-Pirogova, Mateshuk) - a thread passes through the edges of the serous, muscular membranes and submucosa (without capturing the mucous membrane), which ensures good adaptation of the edges and reliable immersion of the mucous membrane into the intestinal lumen without additional traumatization;
double row stitches(Alberta) - used as the first row is a through suture, on top of which (the second row) a serous-muscular suture is applied;
three-row seams– used as the first a series of through sutures, on top of which serous-muscular sutures are applied with the second and third rows (usually used for imposing on the large intestine).
Depending on the characteristics of the sutures through the wall of the wound edge
marginal seams; screw-in seams;
eversion seams; combined screw-in- eversible seams.
According to the overlay method
nodal; continuous.
OPERATIONS ON THE STOMACH
Surgical interventions performed on the stomach are divided into palliative and radical. Palliative operations include: suturing of a perforated gastric ulcer, gastrostomy and gastroenteroanastomosis. Radical operations on the stomach include the removal of part (resection) or the entire stomach (gastrectomy).
Palliative gastric surgery– imposition of an artificial fistula of the stomach
Indications : injured, fistula, burns and cicatricial narrowing esophagus, inoperable cancer of the pharynx, esophagus, cardia of the stomach.
Classification :
tubular fistulas– to create and operate use a rubber tube (Witzel and Strain-ma-Senna-Kader methods); are temporary and usually close on their own after removal of the tube;
labial fistulas– an artificial entrance is formed from the walls of the stomach (the method of Topprover); are permanent, since their closure requires surgery.
Gastrostomy according to Witzel
transrectal left-sided layered laparotomy 10-12 cm long from the costal arch down;
removal of the anterior wall of the stomach into the wound, on which a rubber tube is laid between the small and large curvatures along the long axis, so that its end is located in the pyloric region;
the imposition of 6-8 nodal serous-muscular sutures on both sides of the tube;
immersion of the tube into the gray-serous canal formed by the anterior wall of the stomach by tying sutures;
the imposition of a purse-string suture in the area of the pylorus, opening the wall of the stomach inside the suture, inserting the end of the tube into the cavity of the stomach;
tightening the purse-string suture and applying 2-3 serous-muscular sutures over it;
removal of the other end of the tube through a separate incision along the outer edge of the left rectus muscle;
fixation of the stomach wall (gastropexy) along the formed edge to the parietal peritoneum and to the posterior wall of the sheath of the rectus abdominis muscle with several serous-muscular sutures.
Gastrostomy according to Strain- Senna- Kaderu
transrectal access; removal of the anterior wall of the stomach into the wound and application
closer to the cardia of three purse-string sutures (two in children) at a distance of 1.5-2 cm from each other;
opening the stomach cavity in the center of the internal purse-string suture and inserting a rubber tube;
sequential tightening of purse-string sutures, starting from the inside;
removal of the tube through an additional incision of soft tissues;
gastropexy.
When creating tubular fistulas, it is necessary to carefully fix the anterior wall of the stomach to the parietal peritoneum. This stage of the operation allows you to isolate the abdominal cavity from the external environment and prevent serious complications.
Lipoid gastrostomy according to Topprover
operational access; removal of the anterior wall of the stomach into the surgical wound
in the form of a cone and the imposition of 3 purse-string sutures on it at a distance of 1-2 cm from each other, without tightening them;
dissection of the stomach wall at the top of the cone and introduction of a thick tube inside;
alternately tightening the purse-string sutures, starting from the outside (a corrugated cylinder is formed around the tube from the wall of the stomach, lined with a mucous membrane);
suturing of the stomach wall at the level of the lower purse-string suture to the parietal peritoneum, at the level of the second suture - to
the vagina of the rectus abdominis muscle, at the level of the third - to the skin;
at the end of the operation, the tube is removed and inserted only at the time of feeding.
Gastroenterostomy(an anastomosis between the stomach and small intestine) is performed in violation of the patency of the pyloric part of the stomach (inoperable tumors, cicatricial stenosis, etc.) in order to create an additional path for the removal of gastric contents into the jejunum. Depending on the position of the intestinal loop in relation to the stomach and transverse colon, the following types of gastroenteroanastomoses are distinguished:
anterior anterior colonic gastroenteroanastomosis;
posterior anterior colonic gastroenteroanastomosis;
anterior retrocolic gastroenteroanastomosis;
posterior retrocolic gastroenteroanastomosis. Most often, the first and fourth variants of the operation are used.
When applying the anterior anterior fistula, 30-45 cm recede from the flexura duodenojejunalis (anastomosis for a long
loop) and additionally, in order to prevent the development of a "vicious circle", an anastomosis is formed between the afferent and efferent loops of the jejunum in a side-to-side manner. When applying the posterior retrocolic anastomosis, 7-10 cm recede from the flexura duo-denojejunalis (anastomosis on a short loop). For the correct functioning of the anastomoses, they are applied isoperistaltically (the afferent loop should be located closer to the cardial part of the stomach, and the outlet loop should be closer to the antrum).
Severe complication after the operation of the imposition of the gastrointestinal anastomosis - " vicious circle"- occurs, most often, with an anterior anastomosis with a relatively long loop. The contents from the stomach enters in an antiperistaltic direction into the adductor jejunum (due to the predominance of the motor force of the stomach) and then back to the stomach. Causes This formidable complication is: incorrect suturing of the intestinal loop in relation to the axis of the stomach (in the antiperistaltic direction) and the formation of the so-called "spur".
In order to avoid the development of a vicious circle due to the formation of a "spur", the leading end of the jejunum is strengthened to the stomach by additional serous-muscular sutures 1.5-2 cm above the anastomosis. This prevents the kink of the intestine and the formation of a "spur".
Suturing of a perforated ulcer of the stomach and duodenum
With a perforated gastric ulcer, it is possible to perform two types of urgent surgical interventions: suturing the perforated ulcer or resection of the stomach along with the ulcer.
Indications for suturing a perforated ulcer :
patients in childhood and young age; in individuals with a short ulcer history;
in older people with comorbidities (cardiovascular insufficiency, diabetes mellitus, etc.);
if more than 6 hours have passed since the perforation; with insufficient experience of the surgeon.
When suturing a perforation, it is necessary
adhere to the following rules:
a defect in the wall of the stomach or duodenum is usually sutured with two rows of serous-muscular Lambert sutures;
the suture line should be directed perpendicular to the longitudinal axis of the organ (to avoid stenosis of the lumen of the stomach or duodenum);
radical stomach surgery
Radical operations include gastric resection and gastrectomy. The main indications for these interventions are: complications of peptic ulcer of the stomach and duodenum, benign and malignant tumors of the stomach.
Classification :
Depending on the location of the removed part of the organ:
proximal resections(the cardiac part and part of the body of the stomach are removed);
distal resections(the antrum is removed and body part of the stomach).
Depending on the volume of the removed part of the stomach:
economical - resection of 1/3-1/2 of the stomach;
extensive - resection of 2/3 of the stomach;
subtotal - resection of 4/5 of the stomach.
Depending on the shape of the removed part of the stomach:
wedge-shaped;
stepped;
circular.
Stages of gastric resection
Mobilization(skeletonization) part to be removed-
Ludka– intersection of the vessels of the stomach along the small and greater curvature between the ligatures throughout the resection area. Depending on the nature of the pathology (ulcer or cancer), the volume of the removed part of the stomach is determined.
Resection– the part to be resected is removed stomach.
Restoring the continuity of the digestive tube( gastroduodenoanastomosis or gastroenteroanastomosis ).
In this regard, there are two main types of opera-
The operation according to the Billroth-1 method is the creation of an “end-to-end” anastomosis between the stomach stump and the duodenal stump.
Operation according to the Billroth-2 method - the formation of an anastomosis "side to side" between the stomach stump and the loop of the jejunum, the closure of the duodenal stump ( in class-
not applicable).
The operation according to the Billroth-1 method has an important advantage over the Billroth-2 method: it is physiological, because the natural passage of food from the stomach into the duodenum is not disturbed, i.e. the latter is not switched off from digestion.
However, the Billroth-1 operation can be completed only with “small” resections of the stomach: 1/3 or antrum resection. In all other cases, due to anatomical features (for-
the peritoneal location of most of the duodenum and fixation of the stomach stump to the esophagus), it is very difficult to form a gastroduodenal anastomosis (there is a high probability of suture divergence due to tension).
Currently, for resection of at least 2/3 of the stomach, the Billroth-2 operation is used in the Hofmeister-Finsterer modification. The essence of this modification is as follows:
the stump of the stomach is connected to the jejunum in an end-to-side anastomosis;
the width of the anastomosis is 1/3 of the lumen of the stomach stump;
the anastomosis is fixed in the "window" of the mesentery of the transverse colon;
the adductor loop of the jejunum is sutured with two or three interrupted sutures to the stomach stump to prevent the reflux of food masses into it.
The main disadvantage of all modifications of the Billroth-2 operation is the exclusion of the duodenum from digestion.
In 5-20% of patients who underwent resection of the stomach, diseases of the "operated stomach" develop: dumping syndrome, afferent loop syndrome (reflux of food masses into the afferent loop of the small intestine), peptic ulcers, cancer of the stomach stump, etc. Often such patients have to be operated on again - to perform a reconstructive operation that has two goals: removal of the pathological focus (ulcer, tumor) and inclusion of the duodenum in digestion.
For advanced stomach cancer, gastrek- tomy-removal of the entire stomach. Usually it is removed along with the greater and lesser omentums, the spleen, the tail of the pancreas and regional lymph nodes. After removal of the entire stomach, the continuity of the digestive canal is restored by gastric plasty. Plastic surgery of this organ is performed using a loop of the jejunum, a segment of the transverse rim or other parts of the large intestine. The small or large intestine insert is connected to the esophagus and duodenum, thus restoring the natural passage of food.
Vagotomy- dissection of the vagus nerves.
Indications : complicated forms of duodenal ulcer and pyloric stomach, accompanied by penetration, perforation.
Classification
stem vagotomy– intersection of the trunks of the vagus nerves to the departure of the hepatic and celiac nerves. Leads to parasympathetic denervation of the liver, gallbladder, duodenum, small intestine and pancreas, as well as to gastrostasis (performed in combination with pyloroplasty or other draining operations)
supradiaphragmatic; subphrenic.
Selective vagotomy– is to cross trunks of the vagus nerves, going to the entire stomach, after separation of the branches of the hepatic and celiac nerves.
Selective proximal vagotomy– cross-
Xia branches of the vagus nerves, going only to the body and fundus of the stomach. The branches of the vagus nerves that innervate the antrum of the stomach and the pylorus (Laterje branch) do not cross. The Laterger branch is considered purely motor, which regulates the motility of the saw-
ric sphincter of the stomach.
Draining operations on the stomach
Indications: ulcerative pyloric stenosis, bulbs of the duodenum and the post-bulbous section.
Pyloroplasty – an operation to expand the pyloric opening of the stomach with the preservation or restoration of the closing function of the pylorus.
Heinecke method – Mikulich – lies in pro-
longitudinal dissection of the pyloric part of the stomach and the initial part of the duodenum, 4 cm long, followed by transverse stitching of the formed wound.
Finney's way – dissect the antrum stomach and the initial section of the duodenum with a continuous arcuate incision and
put stitches on the wound according to the principle of the upper gastroduodenoanastomosis "side to side".
Gastroduodenostomy
Jabolei's way – applied if available obstacles in the pyloroanthral zone; a side-to-side gastroduodenoanastomosis is applied, bypassing the place of the obstacle.
Gastrojejunostomy – the imposition of a classic gastroenteroanastomosis on the "off".
Features of the stomach in newborns and children
In newborns, the stomach is rounded, its pyloric, cardiac sections and fundus are weakly expressed. The growth and formation of the sections of the stomach is uneven. The pyloric part begins to stand out only by 2-3 months of a child's life and develops by 4-6 months. The area of the bottom of the stomach is clearly defined only by 10-11 months. The muscular ring of the cardial region is almost absent, which is associated with a weak closure of the entrance to the stomach and the possibility of back throwing of the contents of the stomach into the esophagus (regurgitation). The cardial part of the stomach is finally formed by 7-8 years.
The mucous membrane of the stomach in newborns is thin, the folds are not pronounced. The submucosal layer is rich in blood vessels and has little connective tissue. The muscular layer in the first months of life is poorly developed. The arteries and veins of the stomach in young children differ in that the size of their main trunks and branches of the first and second orders is almost the same.
Malformations
Congenital hypertrophic pyloric stenosis– expressed-
hypertrophy of the muscle layer of the pylorus with narrowing or complete closure of the lumen with folds of the mucous membrane. In the longitudinal direction, the serous membrane and part of the circular muscle fibers of the pylorus are dissected along its entire length, the mucosa of the pylorus is bluntly released from deep muscle fibers until it bulges completely through the incision, the wound is sutured in layers.
constrictions(strictures) body of the stomach– body takes hourglass shape.
Complete absence of the stomach. doubling of the stomach.
Features of the duodenum in newborns- money and children
The duodenum in newborns is more often ring-shaped and less often U-shaped. In children of the first years of life, the upper and lower bends of the duodenum are almost completely absent.
The upper horizontal part of the intestine in newborns is above the usual level, and only by the age of 7-9 falls to the body of the 1st lumbar vertebra. Ligaments between the duodenum and neighboring organs in young children are very tender, and the almost complete absence of fatty tissue in the retroperitoneal space creates the possibility of significant mobility of this section of the intestine and the formation of additional kinks.
Malformations of the duodenum
Atresia– complete lack of light (characterized strong expansion and thinning of the walls of those sections of the intestine that are above the atresia).
stenoses– due to localized hypertrophy of the wall, the presence of a valve, a membrane in the intestinal lumen, compression of the intestine by embryonic cords, an annular pancreas, superior mesenteric artery, and a high-lying caecum.
In case of atresia and stenosis of the jejunum and ileum, the atrezed or narrowed section of the intestine is resected along with a stretched, functionally incomplete area over 20-25 cm. In case of obstruction in the distal intestine, duodenojejunoanastomosis is used.
Diverticula.
Malposition of the duodenum–
mobile duodenum.
Lecture # 7
The upper floor of the abdominal cavity. Organs
The division of the abdominal cavity into floors
The transverse colon and its mesentery form a septum that divides the abdominal cavity into two floors - upper and lower. The division is conditional, because In fact, there is no complete distinction between floors, however, for practical purposes, such a division is convenient (Fig. 1).
The line along which the root of the mesentery of the transverse colon is connected with the posterior abdominal wall runs as follows: on the right, it starts slightly below the level of the middle of the right kidney, then crosses the middle of the descending part of the duodenum, the head of the pancreas, and then passes along the anterior edge of the body of the gland, reaching the left kidneys approximately at the level of its middle. This line approximately corresponds to the transverse line that connects the lower points of the tenth ribs on the anterior abdominal wall.
In the upper floor of the abdominal cavity are: liver, stomach, spleen, pancreas, upper half of the duodenum. The pancreas is located behind the peritoneum; nevertheless, it is considered as an organ of the abdominal cavity, tk. operational access to it is usually carried out by ventricular surgery.
In the lower floor of the abdominal cavity are: loops of the small intestine (with the lower half of the duodenum) and the large intestine.
Derivatives of the peritoneum in the upper floor of the abdominal cavity
In the upper floor of the abdominal cavity, three interconnected bags, or bags, can be distinguished: hepatic (bursa hepatica), pregastric (bursa pregastrica) and omental (bursa omentalis). The first two lie closer to the surface of the abdomen, the third is deep. The hepatic and pregastric bags are separated from each other by the supporting and coronary ligaments of the liver.
The hepatic bursa surrounds the right lobe of the liver, the pregastric bursa is in front of the stomach and surrounds the left lobe of the liver and spleen. The walls of the liver bag are the diaphragm (its costal and lumbar parts) and the anterior abdominal wall; the walls of the pancreatic sac are formed by the diaphragm, the anterior abdominal wall and the stomach with its ligaments.
From top to bottom, each of these bags passes in front of the transverse colon into the preomental space. In addition, the right bag (liver) communicates with the right lateral canal of the abdominal cavity, the left (pregastric) - with the left lateral canal. Communication between both bags is carried out through a narrow gap located between the liver and the pyloric part of the stomach, in front of the lesser omentum.
Stuffing bag
The omental bag, otherwise called the small peritoneal sac, limits a slit-like space located mainly behind the stomach and hepatogastric ligament (Fig. 2, 3).
The bag communicates with the large peritoneal sac through the omental opening - foramen epiploicum (Winslowi). This hole is located near the gate of the liver and is limited in front by the hepatoduodenal ligament, behind - by the inferior vena cava with the peritoneum covering it, from above - by the caudate lobe of the liver, from below - by the initial section of the duodenum.
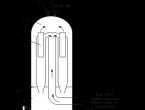
Rice. 1. The course of the peritoneum on the sagittal cut
1 - bladder, 2 - uterus, 3 - transverse colon, 4 - stuffing bag, 5 - preventricular bag, 6 - left hepatic bag, 7 - left coronary ligament, 8 - upper pocket of the stuffing bag, 9 - lesser omentum , 10 - omental opening, 11 - stomach, 12 - duodenum, 13 - greater omentum, 14 - small intestine, 15 - recto-uterine cavity, 16 - rectum.

Rice. 2. Stuffing bag
1 - lesser omentum (omentum minus), 2 - own artery of the liver (a.hepatica propria), 3 - bile duct (ductus choledochus), 4 - portal vein (v.portae), 5 - hepatoduodenal ligament (lig.hepatoduodenal ), 6 - inferior vena cava (v.cava inferior), 7 - aorta (aorta), 8 - kidney (ren), 9 - splenic-renal ligament (lig. splenorenal), 10 - spleen (lien), 11 - gastric - splenic ligament (lig.gastrolienal), 12-stomach (gaster), 13 - splenic pocket (recessus lienalis). (From: Sinelnikov R.D. Atlas of human anatomy. - M., 1972. - T. II.)
In the absence of adhesions (as a result of an inflammatory process in the circumference of the biliary tract, duodenum and pancreas), the omental opening passes more often one, less often two fingers; if adhesions are present, the hole may be closed. During operations on the liver and biliary tract, when there is a need to quickly stop bleeding, the hepatoduodenal ligament with the vessels passing through it can be squeezed with two fingers of the left hand in this way: the thumb is placed on the ligament, and the index finger is inserted into the omental opening behind the ligament.

Rice. 3. Subhepatic and omental bags
1 - right bend of the colon, 2 - upper part of the duodenum, 3 - subhepatic bag, 4 - probe in the omental opening, 5 - gallbladder, 6 - liver, 7 - hepatoduodenal ligament, 8 - esophagus, 9 - gastro- splenic ligament, 10 - spleen, 11 - pancreas, 12 - mesentery of the transverse colon, 13 - left flexure of the colon. (From: Netter F.H. Atlas of human anatomy. - Basle, 1989.)
The ratio of the stuffing box to neighboring organs
The omental bag is limited directly in front and behind by two sheets of peritoneum - anterior and posterior, involved in the formation of the anterior and posterior walls of the bursa omentalis. The anterior leaf of the stuffing bag covers the caudate lobe of the liver from the posterior edge of the organ to the hepatic gate. From here, the anterior leaf goes to the lesser curvature of the stomach, forming the posterior plate of the lesser omentum along the way, then covers the posterior wall of the stomach to its greater curvature and descends, forming the posterior plate of the lig.gastrocolicum. Further, this front sheet, which is the second (inner) plate of the greater omentum, wraps up and forms the third (inner) plate of the greater omentum, then passing into the rear sheet of the stuffing box. This sheet covers the front of the pancreas and reaches the posterior edge of the liver, where it merges with the anterior leaf of the omental sac.
The walls of the stuffing box are; in front - the stomach and the lesser omentum; behind - a sheet of parietal peritoneum covering the pancreas, left kidney, left adrenal gland, aorta, inferior vena cava; below - the left side of the mesentery of the transverse colon; on the left - the spleen with its ligaments; the upper and right walls are not expressed independently. At the top, the cavity reaches the diaphragm, on the right - the duodenum.
If you separate along the greater curvature of the stomach lig.gastrocolicum and pull the stomach up, you can see two folds of the peritoneum stretched between the lesser curvature of the stomach and the anterior surface of the pancreas - plicae gastropancreaticae. One of them, the left one, goes to the pancreas from the lesser curvature of the inlet part of the stomach; a. gastrica sinistra and v. coronaria ventriculi pass in its free edge, and nodi lymphatici gastropancreatici are located in the thickness of the ligament. Another ligament goes to the pancreas from the pyloric part of the stomach and the initial part of the duodenum and contains lymphatic nodules; a.hepatica communis can also pass in it. Between both folds there is a hole - foramen gastropancreaticum. The cavity of the stuffing bag is divided by the indicated folds into two sections - the upper (right) and lower (left), the communication between which is carried out through the foramen gastropancreaticum. The vestibule of the stuffing bag (vestibulum bursae omentalis) belongs to the upper section - the initial section of the cavity, located behind the lesser omentum. Above it there is an upper torsion of the stuffing bag, located behind the caudate lobe of the liver and reaching the esophagus and diaphragm. The lower part of the cavity of the omental bag (the cavity itself), located behind the stomach and gastrocolic ligament, has a lower volvulus, continuing to the left into the splenic volvulus.
The cavity of the stuffing bag also includes a slit-like space enclosed between the leaves of the greater omentum (the cavity of the greater omentum). It exists in newborns, but in adults, usually due to gluing of the sheets of the greater omentum, the slit-like space disappears for most of its length, remaining only in its left section.
subphrenic space
The 3 bags considered (hepatic, pregastric and omental) constitute the intraperitoneal subdiaphragmatic space in contrast to the extraperitoneal subphrenic space located behind the liver. Both subdiaphragmatic spaces play an important role in surgical pathology: abscesses called subdiaphragmatic abscesses can occur here. Intraperitoneal subdiaphragmatic abscesses develop on the basis of damage and diseases of intraperitoneal organs (appendicitis, perforated stomach ulcer, abscesses of the liver and spleen, etc.), and extraperitoneal ones are most often complications of paracolitis and paranephritis.
Liver
The liver (hepar) mostly lies in the right hypochondrium, lesser - in the proper epigastric region and the left hypochondrium.
With its upper surface, the liver adjoins the diaphragm, and its anterior surface adjoins the diaphragm and the anterior abdominal wall. The posterior surface of the liver is adjacent to the X and XI thoracic vertebrae, the crura of the diaphragm, the abdominal esophagus, the aorta, and the right adrenal gland. In the hole on the back of the liver lies v.cava inferior. Part of the posterior surface of the liver is devoid of peritoneal cover and is connected through fibrous tissue with the posterior abdominal wall. This area is called the extraperitoneal field of the liver, which can be wide and narrow. The lower surface of the liver covers the stomach (cardia, lesser curvature, part of the body, antrum, pylorus), the upper horizontal part of the duodenum, its first bend and 1/4 of the descending section; under the liver are also the top of the hepatic curvature of the colon and the upper pole of the right kidney. The gallbladder lies on the lower surface of the liver.
The ligamentous apparatus of the liver consists of: located in the sagittal plane between the upper surface of the liver and the diaphragm, a sickle-shaped, or supporting, ligament (its lower edge contains the round ligament of the liver) and the coronary ligament running along the posterior edge of the liver; it passes on the sides into the right and left triangular ligaments. These formations, related to the peritoneum, connect the liver with the walls of the abdominal cavity. To the organs from the liver go lig.hepatogastricum and hepatoduodenale, which make up the lesser omentum, lig.hepatorenale, there is not always lig.hepatocolicum (Fig. 4).
However, these ligaments do not play a decisive role in the fixation of the liver. Of great importance in this is, firstly, the extraperitoneal field of the liver, and secondly, the inferior vena cava, which lies in a special hole on the posterior surface of the liver and receives the hepatic veins (above the liver, the inferior vena cava is fixed in the opening of the diaphragm); thirdly, the liver is supported from below by the intestines, held under the liver by the pressure of the abdominal muscles.
The liver is covered with peritoneum on all sides, with the exception of the gate and part of the posterior surface (the extraperitoneal field of the liver mentioned above), as a result of which the organ is classified as mesoperitoneal. The parenchyma of the organ is directly covered with a dense fibrous membrane - capsula fibrosa hepatis (Glissoni). It is especially developed in the region of the gate, where it forms the sheaths of the vessels and nerves of the liver.


Rice. 4. Diaphragmatic (a) and visceral (b) surfaces of the liver
1 - attachment of the coronary ligament, 2 - right lobe, 3 - gallbladder, 4 - inferior vena cava, 5 - left lobe, 6 - falciform ligament, 7 - square lobe, 8 - round ligament of the liver, 9 - gap of the venous ligament, 10 - own hepatic artery, 11 - caudate lobe, 12 - portal vein, 13 - common bile duct. (From: Sinelnikov R.D. Atlas of human anatomy. - M., 1972. - T. II.)
Segmental structure of the liver
In connection with the development of liver surgery, its division into lobes according to external signs turned out to be insufficient for practical purposes and does not correspond to the internal structure of the organ. Therefore, studies have appeared that consider the intraorganic structure of the liver, depending on the distribution of blood vessels and bile ducts in it (Fig. 5).
These studies established the coincidence of the course of the branches of the portal vein, the hepatic artery and the bile duct inside the organ within certain sections of the liver (segment).
A.V. Melnikov (1924) was the first to clearly show the presence of isolated circulation zones in the liver, the boundaries of which did not coincide with the accepted division of the organ into lobes according to external signs.
According to the intraorgan branching of the portal vein, hepatic artery and bile ducts, the liver can be divided into 2 lobes, 4 sectors and 8 segments. Segment, sector and lobe are areas of the liver that have to some extent a separate blood supply, bile duct, innervation and lymph circulation.
The boundaries separating the lobes, sectors and segments from each other are low-vascular furrows.
The segments, grouped along the radii around the gates of the liver, are included in larger independent sections of the organ, called sectors. Thus, segments III and IV form the left paramedian sector, the left lateral sector (monosegmental) includes only segment II, the right paramedian sector includes segments V and VIII, the right lateral sector contains segments VI and VII, segment I is the dorsal sector (monosegmental ).
Each lobe, sector or segment of the liver in most cases has a so-called stalk accessible for surgical treatment, in which, closely adjacent to each other, there are branches of the portal vein, hepatic artery and hepatic duct, dressed in a connective tissue sheath.
The approach to the "leg" can be carried out in some cases from the side of the gate of the liver, as well as through the low-vascular furrows.


Rice. 5. Segments of the liver and venous outflow from them
a - venous outflow, b, c - diaphragmatic and visceral surfaces of the liver; 1 - right hepatic vein, 2 - middle hepatic vein, 3 - left hepatic vein, 4 - inferior vena cava, 5 - common hepatic duct, portal vein and own hepatic artery. Roman numerals indicate segment numbers.
A new classification of the intraorgan structure of the liver is important for performing various operations, topical diagnosis of the boundaries of the pathological focus. Resection of the liver, taking into account the distribution of vessels and bile ducts in the segments, sectors and lobes of the liver, avoids a number of complications (bleeding, bile leakage), circulatory disorders and bile outflow in the left part of the organ.
Features of the blood supply to the liver consist in the fact that blood is brought into the organ by two vessels: the hepatic artery and the portal vein (Fig. 6).
Arterial collaterals of the liver vessels are divided into two systems: extraorganic and intraorganic. The extraorganic system is formed mainly by branches extending from a.hepatica communis: aa.gastroduodenalis and gastrica dextra. If the hepatic artery is ligated before the last two vessels depart, then collateral circulation in the liver can be restored.
The intraorgan system of collaterals is formed due to anastomoses between the branches (ramus dexter and sinister) of the liver's own artery.


Rice. 6. Intrahepatic branching of the portal vein, own hepatic artery and bile ducts
The branches of the proper hepatic artery are light, the portal vein is dark, the common hepatic duct is shaded. Roman numerals indicate segment numbers.
However, these anastomoses are often not enough to ensure that when one of the branches is ligated, the collateral circulation of the organ is restored completely. Such ligation, causing necrosis of the liver, is life-threatening.
The portal vein near the gate of the liver is divided into two branches: the right and left, of which the right enters the right lobe of the liver, and the left is divided into two branches, going to the left and middle lobes (square and caudate).
Inside the hepatic branches of the portal vein, the accompanying branches of the hepatic artery and bile ducts, are located in the liver along the spurs of the Glisson (fibrous) capsule and divide the liver into independent vascular segments. There are eight such segments in the liver. Each segment has a stalk consisting of an afferent vein, an artery, and an efferent bile duct. The efferent vessels of the liver (hepatic veins) are located independently of the afferent vessels that form segments.
Outflow of venous blood carried out by hepatic veins vv.hepaticae. More often there are three, less often - four - five (sometimes two). They collect blood that is brought to the liver by both the hepatic artery and the portal vein. The hepatic veins drain into the inferior vena cava immediately below where it passes through an opening in the tendon of the diaphragm into the chest cavity.
Innervation of the liver carried out by the solar plexus, both vagus trunks and the right phrenic nerve. The main nerves of the liver arise from the solar plexus and form the anterior and posterior hepatic plexuses, located between the layers of the hepatoduodenal ligament.
lymph outflow. Superficial efferent lymphatic vessels of the upper surface of the liver and deep vessels accompanying the hepatic veins flow mainly into the lymph nodes of the chest cavity, other efferent vessels of the liver into the nodes of the abdominal cavity. The regional nodes of the first stage for the efferent lymphatic vessels of the liver that flow into the nodes of the abdominal cavity are:
1) hepatic nodes located along a.hepatica communis and a.hepatica propria;
2) nodes lying along the left gastric artery;
3) nodes located in the circumference of the aorta and inferior vena cava.
The main regional nodes of the second stage for the efferent lymphatic vessels of the liver, stomach and pancreas are the celiac nodes adjacent to the trunk of the celiac artery.
Inside the abdominal cavity there is a peritoneal cavity (cavum peritonei), which is a serous sac formed by a continuous transition of the peritoneum from walls to organs, from organs to organs and consisting of a set of slits connected to each other and located between the parietal and visceral layers of the peritoneum. The parietal is called the peritoneum, covering the walls of the abdominal cavity, visceral -abdominal organs. In men, the peritoneal cavity is closed; in women, through the openings of the fallopian tubes, the uterine cavity and the vagina, it communicates with the external environment.
Abdominal organs, covered with the peritoneum on all sides, except for the places of attachment of the mesentery and ligaments (stomach, mesenteric part of the small intestine, transverse colon, etc.), in relation to the peritoneum are located intraperitoneally. The organs covered by the peritoneum on three sides (liver, ascending and descending colons) are located mesoperitoneally in relation to it and protrude into the peritoneal cavity. The organs lying in the retroperitoneal space (pancreas, kidneys, abdominal aorta, etc.), in relation to the peritoneum, are located extraperitoneally, more precisely retroperitoneally, and are covered by the peritoneum mainly in front.
The abdominal cavity is divided by the transverse colon and its mesentery into two floors - upper and lower.
In the upper floor of the abdominal cavity are the liver, stomach with the abdominal part of the esophagus, spleen, upper part of the duodenum. The lower floor houses the small and large intestines. The organs lying in the retroperitoneal space can be located above the level of attachment of the mesocolon transversum (adrenal glands, the beginning of the abdominal aorta, the celiac trunk, the site of the formation of the portal vein, the celiac plexus), above and below this level (kidneys, pancreas, duodenum, aorta, lower vena cava, superior mesenteric artery and vein) and below the level of attachment of the mesentery of the transverse colon (ureters, inferior mesenteric artery and vein, iliac arteries and veins).
Both floors of the abdominal cavity, which make up a single whole, are communicated in front by a gap (spatiuin preepiploicum) located between the omentum and the inner surface of the anterior wall of the abdomen, and on the sides - through lateral canals.
If, after removal of the anterior wall of the abdomen, you look at the upper floor of the abdominal cavity, then it is clear that in the epigastric region, from under the costal arches and the xiphoid process, the anteroinferior edge of the left and right lobes of the liver protrudes. At the level of the intersection of the costal arch with the outer edge of the right rectus abdominis muscle, the bottom of the gallbladder is located. Below the liver, the lower part of the lesser omentum is sometimes visible. Here lie the upper part of the duodenum, the pyloric part and the lower right part of the body of the stomach. The greater omentum hangs down from the greater curvature of the stomach. The main mass of the liver, part of the body and the fundus of the stomach, the abdominal part of the esophagus and the spleen are located under the diaphragm behind the lower anterior chest.
When the peritoneum passes from the walls of the abdominal cavity to the abdominal organs and from organ to organ, it forms folds and ligaments.
Rice. 120. View of the right half of the abdominal cavity and pelvic cavity on the median sagittal cut (1/8).
From the upper surface of the liver to the diaphragm and the anterior abdominal wall, the peritoneum passes in the form of a thin obliquely located lig. falciforme hepatis, which runs almost from the navel up to the level of the posterior surface of the liver, where it continues in front of the inferior vena cava into the coronary ligament of the liver. In the lower part of the falciform ligament is located lig. teres hepatis (obliterated v. umbilicalis). Lig. coronarium hepatis, passing from the liver to the diaphragm and the inferior vena cava, limits the back of the liver, not covered by the peritoneum (extraperitoneal subphrenic space). Along the edges, the coronary ligament passes into ligg. triangularia dextrum and sinistrum. From the gate of the liver peritoneum in the form of lig. hepatogastricum and lig. hepatoduodenale, which together make up the lesser omentum (omentum minus), passes to the lesser curvature of the stomach and the upper part of the duodenum. Lig. hepatorenale goes from the back of the margo inferior of the right lobe of the liver to the upper pole of the right kidney.
Enveloping the stomach in front and behind, the visceral sheets of the peritoneum are connected at its greater curvature and, bypassing the transverse colon, go down in the form of a greater omentum (omentum majus).
At the free edge of the latter, the leaves tuck back and return upward to the transverse colon, where they fuse with it along the taenia omentalis, and above - with the anterior superior surface of the mesocolon transversum, at the base of which the upper of the leaves continues into the parietal peritoneum of the posterior wall of the cavum peritonei. Below the transverse colon in newborns, between the descending and ascending sheets of the greater omentum, there is a cavity, which then overgrows, and the greater omentum in adults is 4 fused sheets of the visceral peritoneum. Above the transverse colon, the greater omentum consists of. 2 sheets and, since it connects the greater curvature of the stomach with the transverse colon, this section is called lig. gastrocolicum. Up and to the left, the gastrocolic ligament continues in lig. gastrolineale, which is located between the fundus of the stomach and the gates of the spleen. The outer sheet of the peritoneum of this ligament covers the spleen and, meeting on the other side of the gate of the spleen with the inner sheet, continues as lig. phrenicolienale. Even higher, the gastro-splenic ligament passes into lig. gastrophrenicum, which connects the cardial part of the stomach with the diaphragm.
Stuffing bag(bursaomentalis) is located behind the lesser omentum and stomach, which serve as the front wall of the bag. The other walls of the bag are: behind - the parietal peritoneum, covering the front of the pancreas, inferior vena cava, left adrenal gland, part of the upper pole of the left kidney, diaphragm, celiac trunk and its branches; above - the caudate lobe of the liver and the vault, which forms the parietal peritoneum of the posterior wall of the bag during the transition to the liver (part of the coronary ligament), esophagus and stomach (lig. gastrophrenicum); below - the transverse colon and its mesentery; on the left - the gate of the spleen and lig. gastrolienale and lig. phrenicolienale; on the right - a fold of the peritoneum, formed during the transition of the parietal peritoneum of the posterior wall to the duodenum and gastrocolic ligament. In the upper part of the right wall there is an omental (Winslov) opening (foramen epiploicum), which communicates the cavity of the bag with the other, most of the upper floor of the peritoneal cavity. The hole, which passes 1-2 fingers in the absence of adhesions, is limited: in front - by the hepatoduodenal ligament, in the back - by the parietal peritoneum covering the inferior vena cava, from above - by the caudate lobe of the liver and the arch that forms the peritoneum during the transition from lig. hepatoduodenale on the liver, below - the upper edge of the upper part of the duodenum.

Rice. 121. The upper floor of the abdominal cavity. Front view.
Removed the anterior abdominal wall, anterior chest and diaphragm. The diaphragm is pulled up.
On the back wall of the omental bag there are folds of the peritoneum (plicae gastro-pancreaticae), from which the left, upper, formed due to the protrusion of the peritoneum over the left gastric artery, goes to the lesser curvature of the stomach, and the right, lower, formed due to the protrusion of the peritoneum over the common hepatic artery, goes to the hepatoduodenal ligament. The part of the omental bag between the folds and the omental opening is called the vestibule (vestibulum bursae omentalis). Above the vestibule, behind the caudate lobe of the liver, is the recessus superior omentalis; downward, between the posterior surface of the stomach and the gastrocolic ligament in front and the omental tubercle of the pancreas and the mesocolon transversum in the back, there is a recessus inferior omentalis. To the left of the vestibule lies the recessus lienalis.
In addition to the stuffing box, in the upper floor of the abdominal cavity, bursa hepatica and bursa pregastica are also distinguished. The hepatic bag is located between the diaphragm from above and flexura coli dextra and the upper part of the duodenum from below. The bag contains the right lobe of the liver. In front, it is limited by the anterior abdominal wall, covered by the parietal peritoneum. Between the diaphragmatic surface of the right lobe of the liver and the diaphragm there is a slit-like right subphrenic space, and between its visceral surface and the right bend of the colon and the upper part of the duodenum there is a subhepatic slit-like space.
Both of these gaps, as well as the gap between the right lobe of the liver and the anterior abdominal wall, constitute the hepatic sac. In the downward direction, the bag passes into the right lateral canal and preomental gap; in the medial direction through the omental opening, it communicates with the bursa omentalis.

Rice. 122. Small omentum, stuffing bag and stuffing box (Winslov) hole. Upper abdominal organs. Front view.
The same as in fig. 121. In addition, the stomach, the middle part of the transverse colon and its mesentery, and part of the lesser omentum were removed.
The pancreatic bag is located between the diaphragm at the top and the anterior wall of the stomach and flexura coli sinistra and lig. phrenicocolicum at the bottom. In front, it is limited by the anterior abdominal wall, covered by the parietal peritoneum. The bag contains the left lobe of the liver and spleen. From top to bottom, the pancreatic sac passes into the left lateral canal and preomental fissure. The falciform ligament of the liver separates both bags. Below the liver, the bags communicate with each other through a gap located between the liver and lig. teres hepatis in front and above and the pyloric part of the stomach and the lesser omentum behind and below. Together, the three bags described above form an intraperitoneal subphrenic space, within which abscesses can develop as complications after perforation of gastric and duodenal ulcers, after appendicitis, paracolitis, paranephritis, etc.
The lower floor of the abdominal cavity is located below the transverse colon and its mesentery and is more or less closed in front by a large omentum hanging from the greater curvature of the stomach. After retraction of the greater omentum, and with it the transverse colon upwards, the lower floor of the abdominal cavity opens completely. It is made by loops of the small intestine, along the edges and behind which are the ascending and descending parts of the colon. The jejunum and ileum, the vermiform appendix, the cecum, the transverse colon and the sigmoid colon, in addition to the places where the mesentery is fixed to them, are covered with peritoneum from all sides. The ascending and descending parts of the colon are covered by the peritoneum, usually on three sides, except for the posterior surface. If the loops of the small intestine are taken aside or removed, then between the colon ascendens and colon descendens and the lateral walls of the abdomen, the right and left lateral canals connecting the upper floor of the abdominal cavity with the iliac fossae become clearly visible. The left lateral canal, thanks to the constantly present lig. phrenicocolicum, is more isolated from the upper abdominal cavity than the right one, where the same ligament is absent in most cases. However, the right lateral canal at the level of the caecum may be interrupted to some extent by the plicae caecales. Through the lateral canals (especially the right one), when a gastric or duodenal ulcer perforates, gastric and intestinal contents can penetrate into the iliac fossae, and from there into the small pelvis. Pus and blood can spread along the side channels in both directions.

Rice. 123. Topography of the organs of the chest and abdominal cavities on a horizontal cut. View from above.
The cut was made at the level of the X thoracic vertebra.
Inward from the ascending and descending parts of the colon, to the right and left of the root of the mesentery of the small intestine, the right and left mesenteric sinuses are located. The right mesenteric sinus (sinus mesentericus dexter) is smaller in area than the left and is limited: on the right - by the ascending colon, on the left and below - by the root of the mesentery of the small intestine, from above - by the mesentery of the transverse colon. The left mesenteric sinus (sinus mesentericus sinister) is limited: above - by the mesentery of the transverse colon, on the right - by the root of the mesentery of the small intestine, on the left - by the descending colon, and on the left and below - by the mesentery of the sigmoid colon. The left sinus is more extensive and somewhat elongated in an oblique direction, from left to right and from top to bottom.
To the right of the rectum, the left sinus passes directly into the pelvic cavity. Between themselves, the sinuses communicate at the top with a gap between the mesocolon transversum and the beginning of the jejunum.
The deepest are the lateral sections of the sinuses at the medial edges of the ascending and descending parts of the colon.
However, the deepest areas on the posterior wall of the abdominal cavity, along with the posterior sections of the right and left subdiaphragmatic spaces, are the lateral canals. In them, just as in the mesenteric sinuses and in the cavity of the small pelvis, free fluid (pus, blood, transudate) can accumulate.
Peritoneal pockets can be the site of internal hernias. The most constant are those located in the right iliac fossa, above and below the confluence of the ileum in the caecum, recessus ileocaecalis superior and recessus ileocaecalis inferior; recessus retrocaecalis is found behind the caecum. He less often there are pockets of the peritoneum between the flexura duodeno-jejunalis and plica duodenojejunalis - recessus duodenalis superior and at the base of the mesocolon sigmoideum - recessus intersigmoideus.
Related content: